Education - Primary Ovarian Insufficiency
Why Primary Ovarian Insufficiency (POI) Should Be Recognized as a Multi-System Condition Similar to PMOS/PCOS
Why Primary Ovarian Insufficiency deserves the same attention we now give PCOS - and why every woman, every clinician, and every health system needs to take it seriously.
By Dr. Vaishali Popat, MD, MPH - Vital Endocrinology
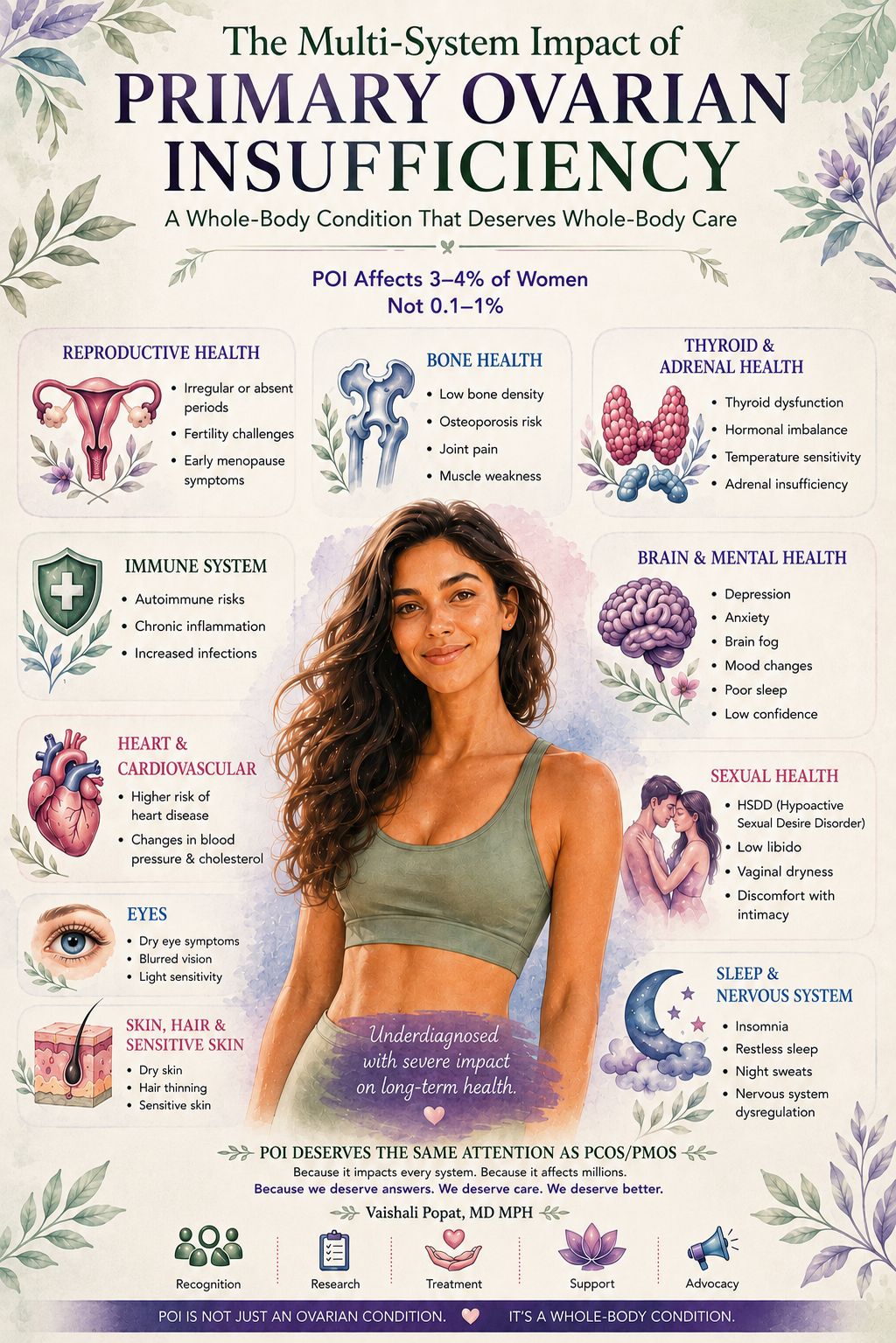
A whole-body condition: what POI actually touches
If you only remember one thing about POI, remember this: it is the whole body, not just the ovaries.
Reproductive system
Irregular or absent periods are often the first sign - easily dismissed in young women as "stress" or "pill side effects."
Infertility is the headline diagnosis for many women, but spontaneous pregnancy is still possible in 5-10% of cases.2
Vaginal and vulvar tissues become dry, thin, and fragile, leading to discomfort, recurrent irritation, and painful sex (dyspareunia).
Bone health
Cardiovascular health
Thyroid and adrenal glands
Thyroid autoimmunity is the most common autoimmune association in POI. Published reviews report thyroid autoimmune disease or thyroid antibody positivity in approximately 14-32.7% of women with POI, while overt or subclinical thyroid dysfunction is reported in roughly 8-20%, depending on the cohort and definitions used.10
A much smaller but important subset develops autoimmune adrenal insufficiency (positive 21-hydroxylase antibodies) - a condition that can be life-threatening if missed, which is why we screen for it.1,10
Brain, mood, and cognition
Skin, hair, and connective tissue
Estrogen has a major supportive effect on collagen. In simple terms, it helps the body make, maintain, and protect collagen-rich tissues, especially in the skin, connective tissue, bone, blood vessels, and urogenital tissues. When estrogen levels fall, collagen production tends to decline and collagen breakdown tends to increase. Without it, skin becomes dry, hair thins, wound healing slows, and joints can ache.
Sexual function and quality of life
Low libido, painful intercourse, and the emotional weight of an infertility diagnosis in a young woman compound into a quality-of-life impact that is too often left unaddressed.9
The cost of delay is real. Every year without treatment is bone loss, vascular stiffening, and cognitive change that does not fully reverse later.
What needs to change
If PCOS is finally getting the recognition it deserves as a whole-body metabolic-endocrine syndrome, POI deserves the same. A few things would help:
- Train more clinicians - primary care, OB/GYN, endocrinology, and adolescent medicine - to recognize POI early and to manage it across the lifespan.
- Update guidelines and patient education materials to reflect the new prevalence data: this is not a 1% condition.
- Fund research into causes, biomarkers, and ovarian regeneration. Stem cell and gene therapy approaches are early but real.
- Treat POI as the public health issue it is, especially in the context of declining fertility rates and rising maternal age.
- Listen to patients. Their lived experience is more accurate than the textbook estimate of "rare."
A note to women who suspect they may have POI
If your periods have become irregular or stopped before age 40, if you are experiencing hot flashes or night sweats in your 20s or 30s, if you are struggling to conceive, or if a sister or mother has had early menopause, ask to be evaluated. The workup is straightforward: two FSH levels two weeks apart, estradiol, TSH, AMH, prolactin, karyotype, FMR1 testing, and adrenal antibodies are the foundation. Imaging may be added.1,15
And if you are told nothing can be done - please get a second opinion. There is a great deal that can be done, and you deserve a clinician who knows how to do it.
Different bodies. Different symptoms. Same need for answers.
POI deserves recognition. POI deserves research. POI deserves real care.
Considering a consultation?
Dr. Vaishali Popat sees women with POI virtually across Maryland, Florida, and Virginia.
This article is for educational purposes only and does not constitute medical advice. Please consult a qualified physician for personalized guidance.
References
- 1. Franca MM, Mendonca BB. Primary ovarian insufficiency: update on clinical and genetic findings. Frontiers in Endocrinology. 2024;15:1464803. doi:10.3389/fendo.2024.1464803. View source
- 2. Nelson LM. Primary ovarian insufficiency. New England Journal of Medicine. 2009;360(6):606-614. doi:10.1056/NEJMcp0808697. View source
- 3. Coulam CB, Adamson SC, Annegers JF. Incidence of premature ovarian failure. Obstetrics & Gynecology. 1986;67(4):604-606. Historical 1% estimate. View source
- 4. Golezar S, Ramezani Tehrani F, Khazaei S, Ebadi A, Keshavarz Z. The global prevalence of primary ovarian insufficiency and early menopause: a meta-analysis. Climacteric. 2019;22(4):403-411. doi:10.1080/13697137.2019.1574738. View source
- 5. Li M, Zhu Y, Wei J, et al. The global prevalence of premature ovarian insufficiency: a systematic review and meta-analysis. Climacteric. 2023;26(2):95-102. doi:10.1080/13697137.2022.2153033. View source
- 6. Lass-Hennemann J, et al. Primary ovarian insufficiency: nationwide incidence rate and etiology among Israeli adolescents. Journal of Adolescent Health. 2020;66(5):603-609. View source
- 7. Liu PY, Beilin J, Meier C, Nguyen TV, Center JR, Leedman PJ, Seibel MJ, Eisman JA, Handelsman DJ. The overlooked and undertreated perils of premature ovarian insufficiency. Cleveland Clinic Journal of Medicine. 2025;92(8):475-484. View source
- 8. Popat VB, Calis KA, Vanderhoof VH, et al. Bone mineral density in estrogen-deficient young women. Journal of Clinical Endocrinology & Metabolism. 2009;94(7):2277-2283. doi:10.1210/jc.2008-1878. View source
- 9. Webber L, Davies M, Anderson R, et al. ESHRE guideline: management of women with premature ovarian insufficiency. Human Reproduction. 2016;31(5):926-937. doi:10.1093/humrep/dew027. View source
- 10. Silva CA, Yamakami LYS, Aikawa NE, et al. Autoimmune primary ovarian insufficiency. Autoimmunity Reviews. 2014;13(4-5):427-430. doi:10.1016/j.autrev.2014.01.003.
- 11. Sherman SL, Curnow EC, Easley CA, et al. Fragile X-associated primary ovarian insufficiency (FXPOI). National Library of Medicine - MedlinePlus Genetics. Updated 2024. View source
- 12. Persani L, Rossetti R, Cacciatore C. Genes involved in human premature ovarian failure. Journal of Molecular Endocrinology. 2010;45(5):257-279. View source
- 13. Sullivan SD, Sarrel PM, Nelson LM. Hormone replacement therapy in young women with primary ovarian insufficiency and early menopause. Fertility and Sterility. 2016;106(7):1588-1599. doi:10.1016/j.fertnstert.2016.09.046. View source
- 14. Kodaman PH. Hormone replacement therapy for women with premature ovarian insufficiency: a comprehensive review. Human Reproduction Open. 2017;2017(2):hox007. doi:10.1093/hropen/hox007. View source
- 15. American College of Obstetricians and Gynecologists. Committee Opinion No. 698: Hormone Therapy in Primary Ovarian Insufficiency. Obstetrics & Gynecology. 2017;129(5):e134-e141. Reaffirmed 2020. View source
- 16. ESHRE Guideline Group on POI; Webber L, et al. Evidence-based guideline: premature ovarian insufficiency (2024-2025 update). American Society for Reproductive Medicine / Human Reproduction. 2024. View source